{kind=link}
Eshealthtips.com – The indications for Gastric Biopsy and the sampling patterns vary considerably between centers. Centers that routinely apply the updated Sydney classification and those that only refer patients with suspected ulcers had fewer biopsies performed than centers that stratified patients using the OLGA system. In contrast, centers that follow MAPS guidelines for stomach surveillance had more biopsies performed. The study’s findings suggest that a change in sampling pattern may not have a significant effect on the need for a matched biopsy.
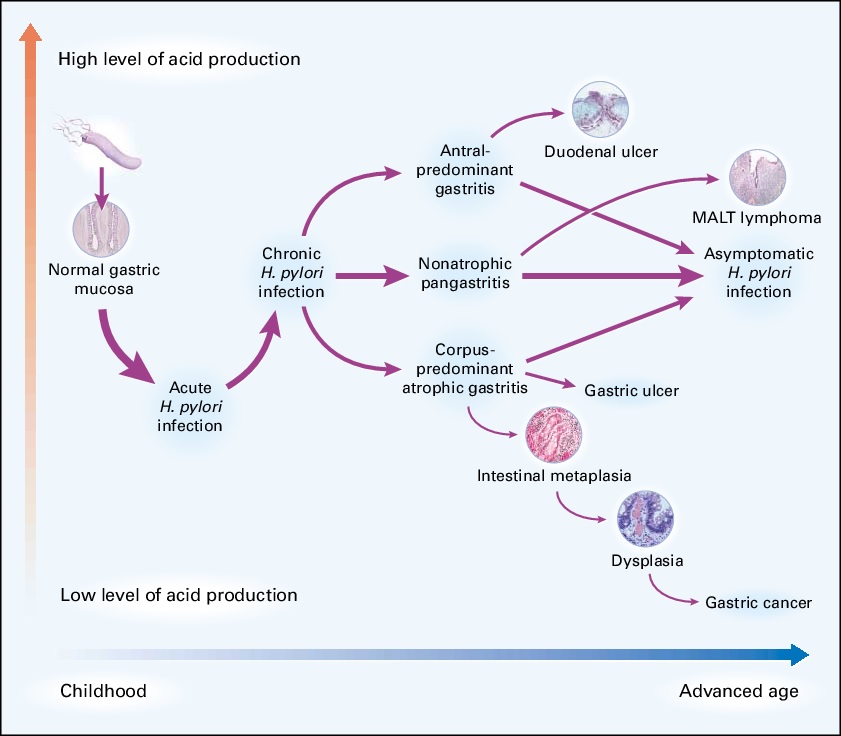
Bacterial Infections of the Stomach
The high level of infection in the antrum may be an indicator of H. pylori or another gastric disease, although a normal gastric mucosa does not necessarily indicate a risk of either. Performing routine gastric biopsies may also uncover special forms of gastritis, such as eosinophilic, lymphocytic, and reactive gastritis. In addition, some patients may have Helicobacter heilmannii gastritis, a bacterial infection of the stomach.
While guidelines recommend that biopsy should be done whenever there is an endoscopic suggestion of inflammation, they are often arbitrary. To determine whether biopsy practices are accurate, a study of ten tertiary referral centers across Europe was undertaken. Researchers analyzed demographic data, endoscopic findings, and biopsy procedures. The results showed that biopsies were performed in 56.6% of 9,425 procedures, with gastric biopsies accounting for 43.8% of all procedures.

In a recent study, a large number of patients with suspected gastric neoplasms underwent biopsy procedures. In contrast to patients without a gastric neoplasm, biopsies were performed on 31.4% of patients. However, biopsies performed on patients with CLO testing were more likely to occur in patients with gastric inflammation. Consequently, the procedure’s success rate was higher in patients with gastric inflammatory diseases.
Diagnosing Asymptomatic or Recurrent Cancer
However, gastric biopsy specimens should be screened for abnormality by pathologists. Thicker folds yield higher yields than erosions, which decrease the yield. Erosions are associated with more errors, and must be carefully ruled out. For instance, gastric biopsy specimens with a high rate of recurrence may be falsely interpreted. Consequently, gastric biopsy specimens should not be used to diagnose asymptomatic or recurrent cancer.
During this procedure, the endoscope is inserted into the mouth and the stomach through the food pipe. The doctor may also perform an EGD during this procedure. A small camera called an endoscope is used to view the area. The sample of tissue will be sent to a laboratory for analysis. After the biopsy, a pathologist will confirm whether or not it is a malignant tumor. The sample can also reveal any other problems that could be present in the gastric tissue.

Immunohistochemical analysis of gastric biopsy specimens is useful for identifying the presence of Helicobacter pylori. However, there are some conditions where this diagnostic tool can be difficult to detect. In particular, biopsy specimens with few samples that are difficult to obtain may not be correctly diagnosed. In such cases, the use of immunohistochemical stains may prove useful. In addition, it may be difficult to distinguish between atrophic gastritis.
Identifying Inflammatory Gastric Conditions
The most common indications for gastric biopsy are to detect Helicobacter pylori infection or to identify a stomach inflammatory condition. In the same vein, gastric biopsy is also used to quantify the gastric mucosal endocrine cell populations. Additionally, biopsy specimens may also reveal gastritis, atrophy, and Helicobacter pylori. There are several factors to consider when undergoing gastric biopsy.
Endoscopic surveillance of gastric lesions has become an effective way to detect early-stage disease and reduce mortality. However, it is still not widely used in the western world. This is primarily because of technical and biological issues. In addition, preneoplastic changes are more difficult to detect and are more subtle. The aim of the gastric biopsy is to identify and manage the disease and its symptoms. There are no guarantees that a biopsy will be accurate, but if it does, the risk of cancer is greatly reduced.
The diagnostic yield of a gastric biopsy depends on the site of the specimen and the number of serial biopsies. The cumulative sensitivity of a biopsy-based on serial biopsies was 95% after the fourth biopsy. The cumulative sensitivity increased to 100% with the fifth biopsy. This was achieved after stratifying biopsies according to gross morphology. Overall diagnostic yield was 144/145 (99.3%) and 144/145 (100%) for depressed/ulcer lesions, respectively.
Reference: